Rev’s Transcript Library
Explore our extensive collection of free transcripts from political figures and public events. Journalists, students, researchers, and the general public can explore transcripts of speeches, debates, congressional hearings, press conferences, interviews, podcasts, and more.

Trump Event in Las Vegas
Donald Trump delivers remarks in a Las Vegas casino. Read the transcript here.

Abdul El-Sayed Wins Michigan Senate Primary
Abdul El-Sayed holds a press conference following his victory in the Democratic primary for Michigan’s U.S. Senate seat. Read the transcript here.

Senate Hearing on Surveillance Pricing
The Senate Judiciary Committee holds a hearing on the impacts of AI surveillance pricing on consumers. Read the transcript here.


Executive Orders 8/03/26
Donald Trump signs executive orders at the White House on 8/03/26. Read the transcript here.

Cabinet Meeting at Camp David 7/31/26
Donald Trump holds a meeting of his cabinet at Camp David on 7/31/26. Read the transcript here.


AI Effects on Workforce Hearing
Senate HELP subcommittee holds hearing on AI’s effect on the workforce. Read the transcript here.

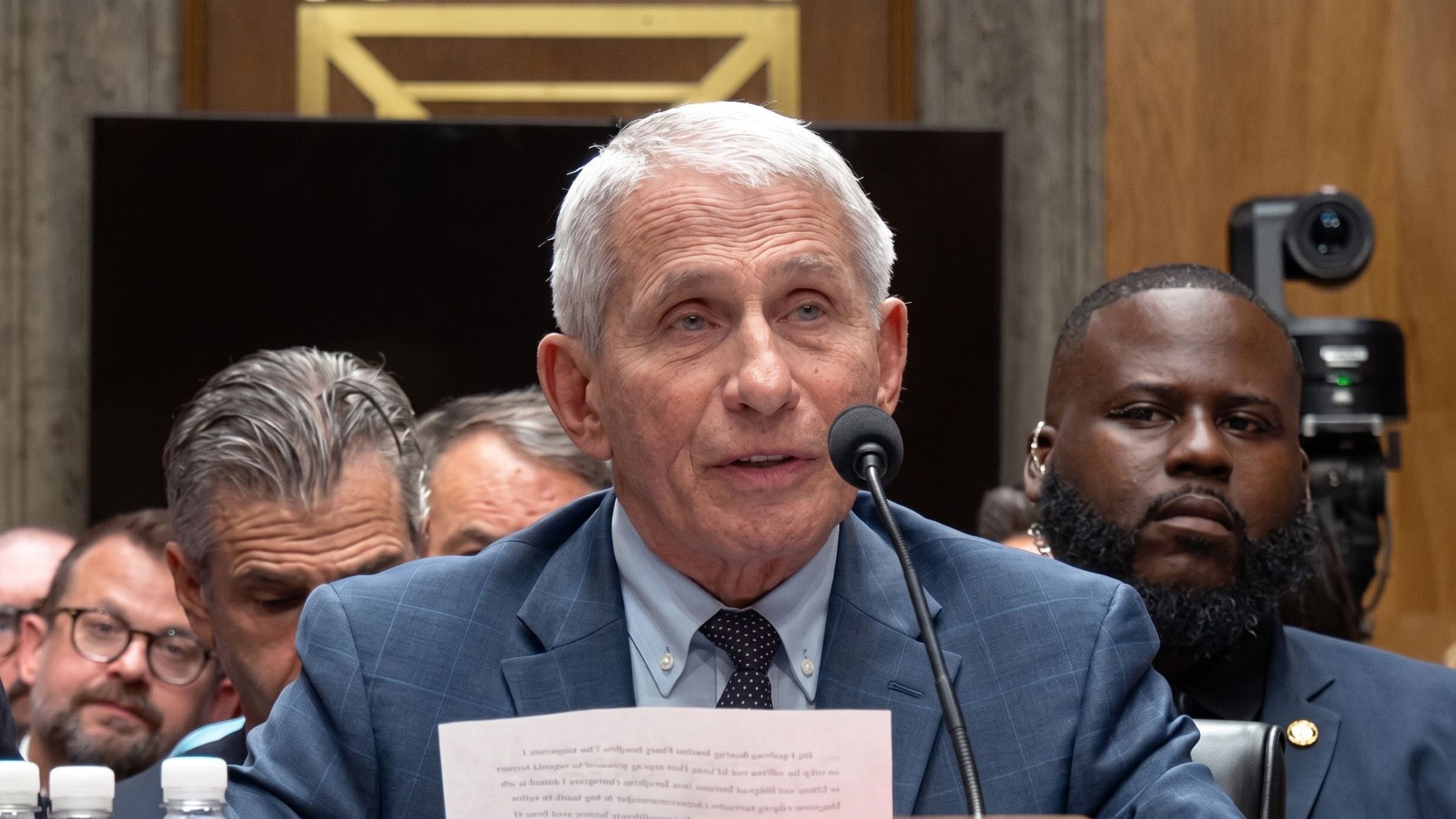
Fauci Congressional Hearing
The Senate Homeland Security Committee holds a hearing to take the testimony of Dr. Anthony Fauci. Read the transcript here.
Subscribe to The Rev Blog
Sign up to get Rev content delivered straight to your inbox.