Rev’s Transcript Library
Explore our extensive collection of free transcripts from political figures and public events. Journalists, students, researchers, and the general public can explore transcripts of speeches, debates, congressional hearings, press conferences, interviews, podcasts, and more.


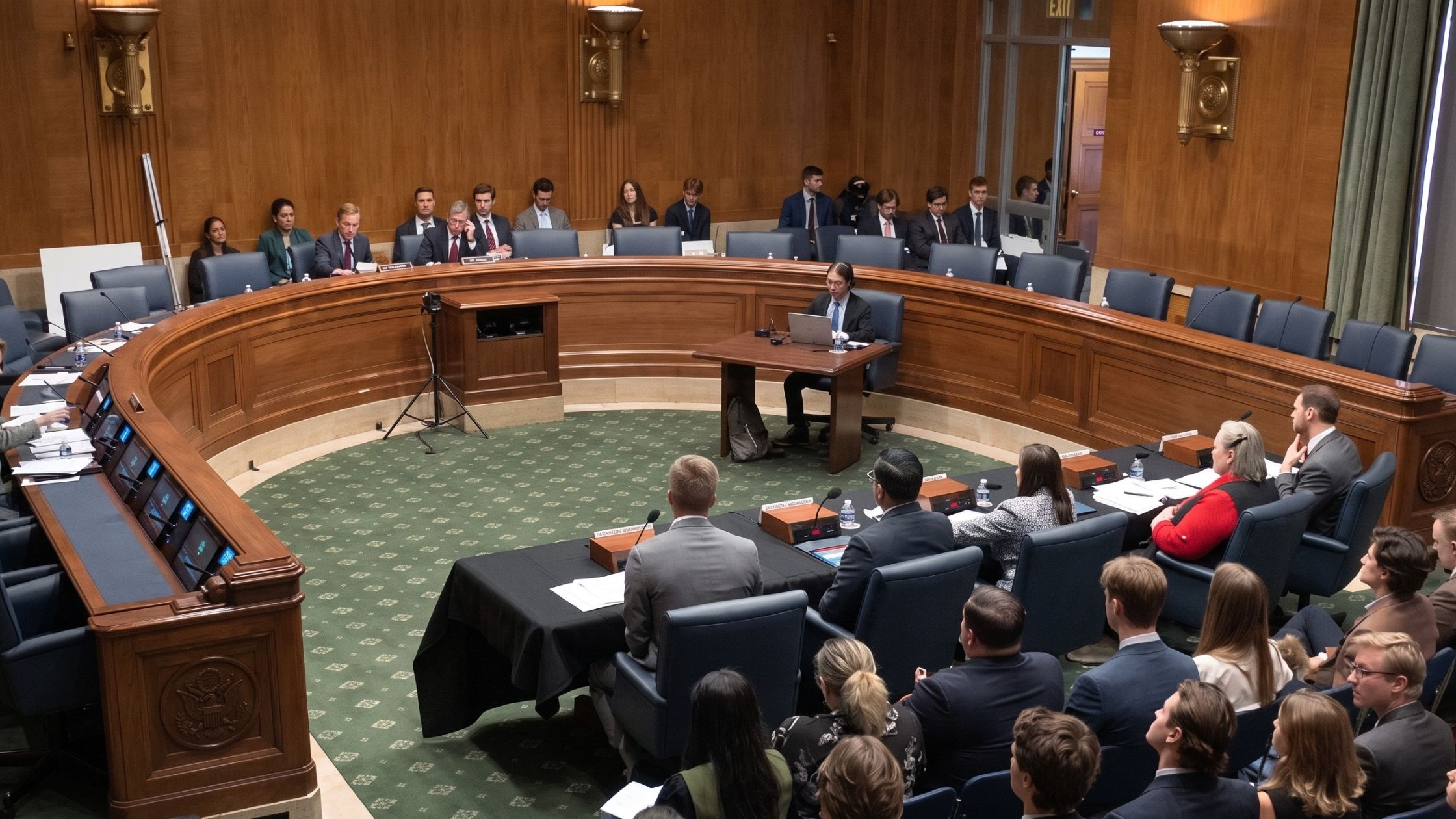
AI Effects on Workforce Hearing
Senate HELP subcommittee holds hearing on AI’s effect on the workforce. Read the transcript here.

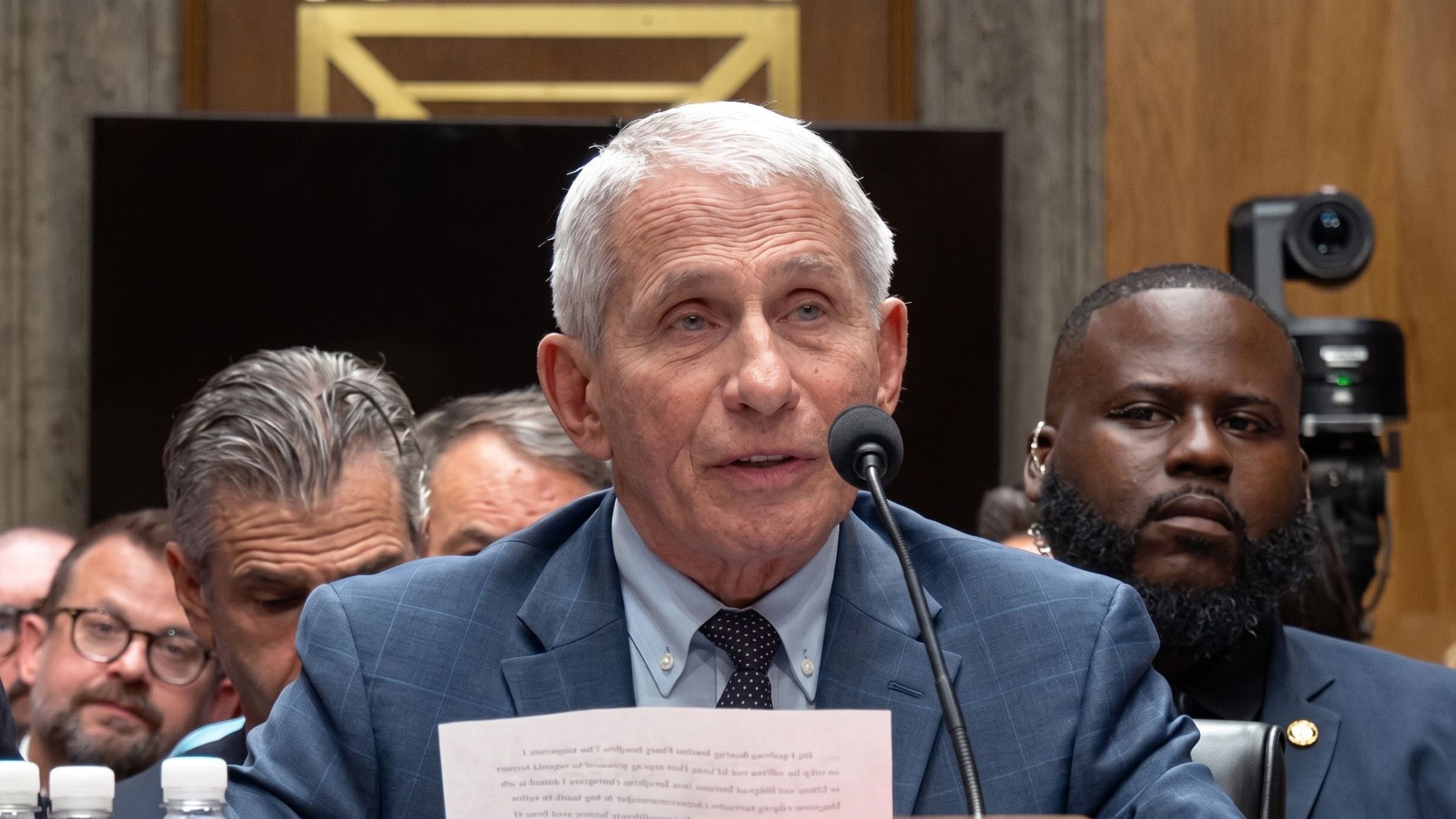
Fauci Congressional Hearing
The Senate Homeland Security Committee holds a hearing to take the testimony of Dr. Anthony Fauci. Read the transcript here.

Funeral for Lindsey Graham
Funeral service for Senator Lindsey Graham at Washington National Cathedral. Read the transcript here.

MA v. Lindsay Clancy Opening Statements
Opening arguments in the murder trial of Lindsay Clancy. Read the transcript here.
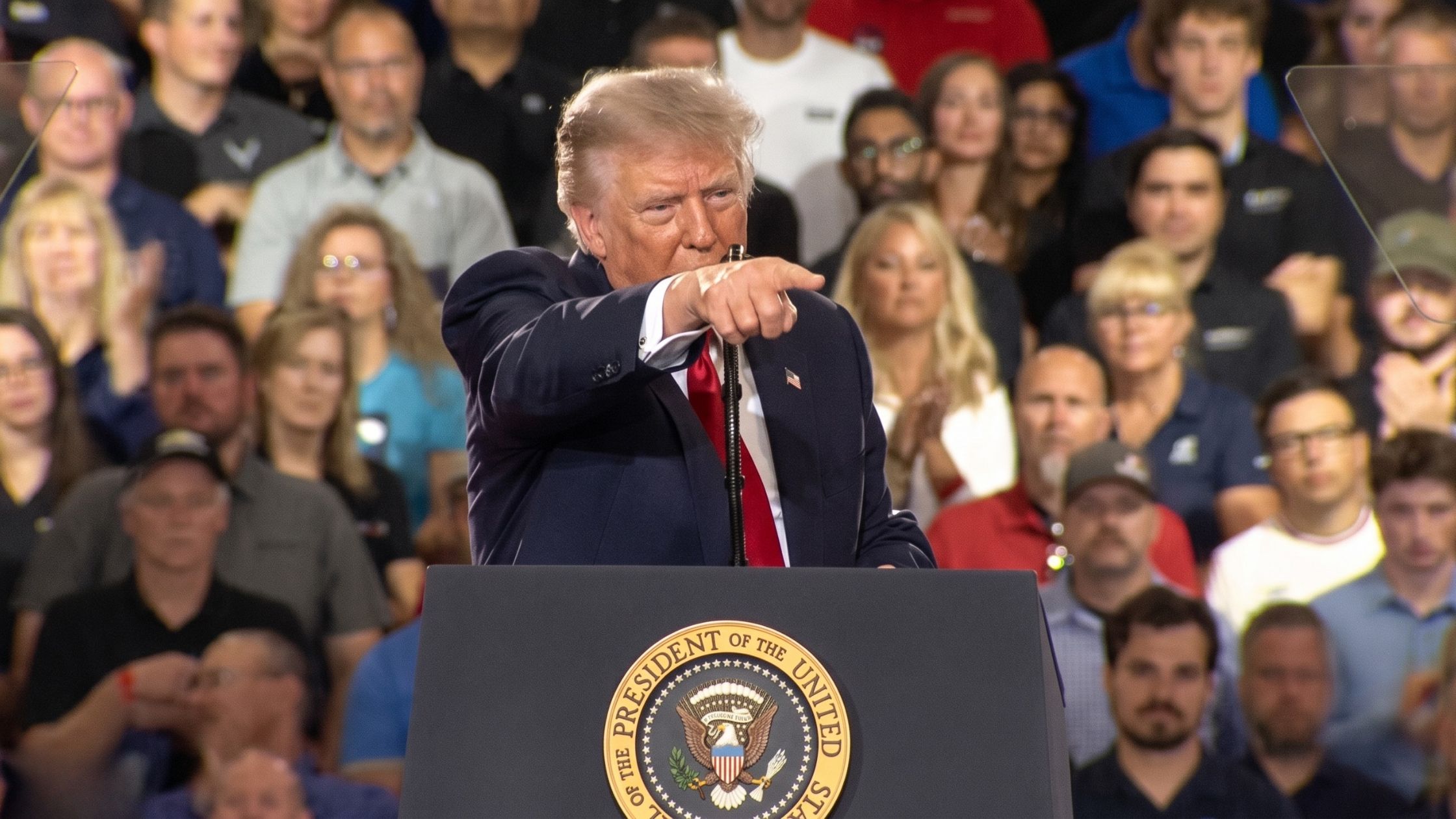
Trump Rally on 7/27/26 in Michigan
Donald Trump holds an event in Michigan on 7/27/26. Read the transcript here.

White House Correspondants Dinner
Donald Trump speaks at the White House Correspondents' Dinner. Read the transcript here.

Seattle Shooting Press Conference
Officials give an update on the Seattle Center shooting near the Space Needle. Read the transcript here.


Subscribe to The Rev Blog
Sign up to get Rev content delivered straight to your inbox.