Rev’s Transcript Library
Explore our extensive collection of free transcripts from political figures and public events. Journalists, students, researchers, and the general public can explore transcripts of speeches, debates, congressional hearings, press conferences, interviews, podcasts, and more.
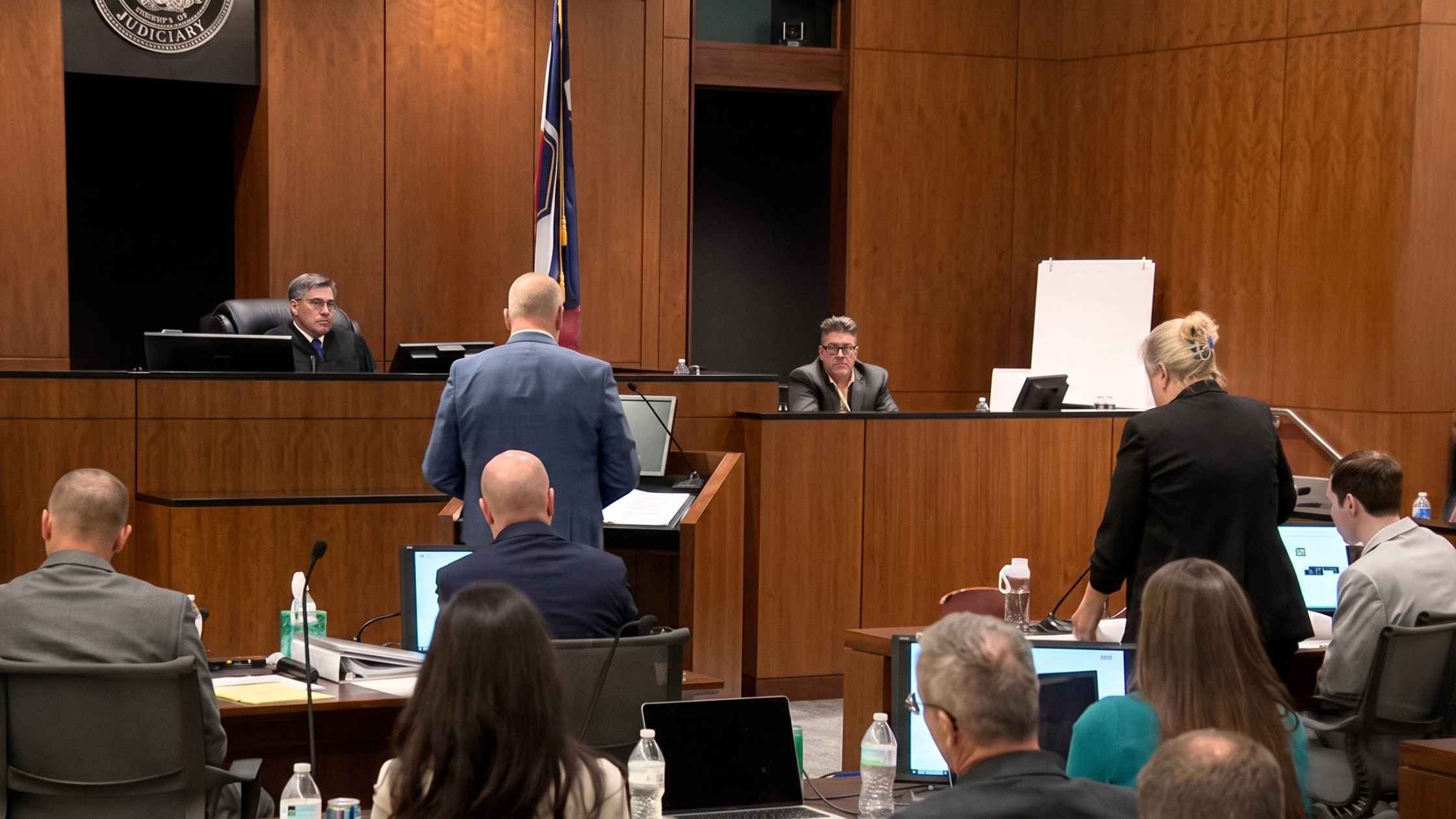
UT v. Tyler Robinson Preliminary Hearing Day 1
Charlie Kirk's accused killer, Tyler Robinson, is in court as prosecutors begin a preliminary hearing. Read the transcript here.
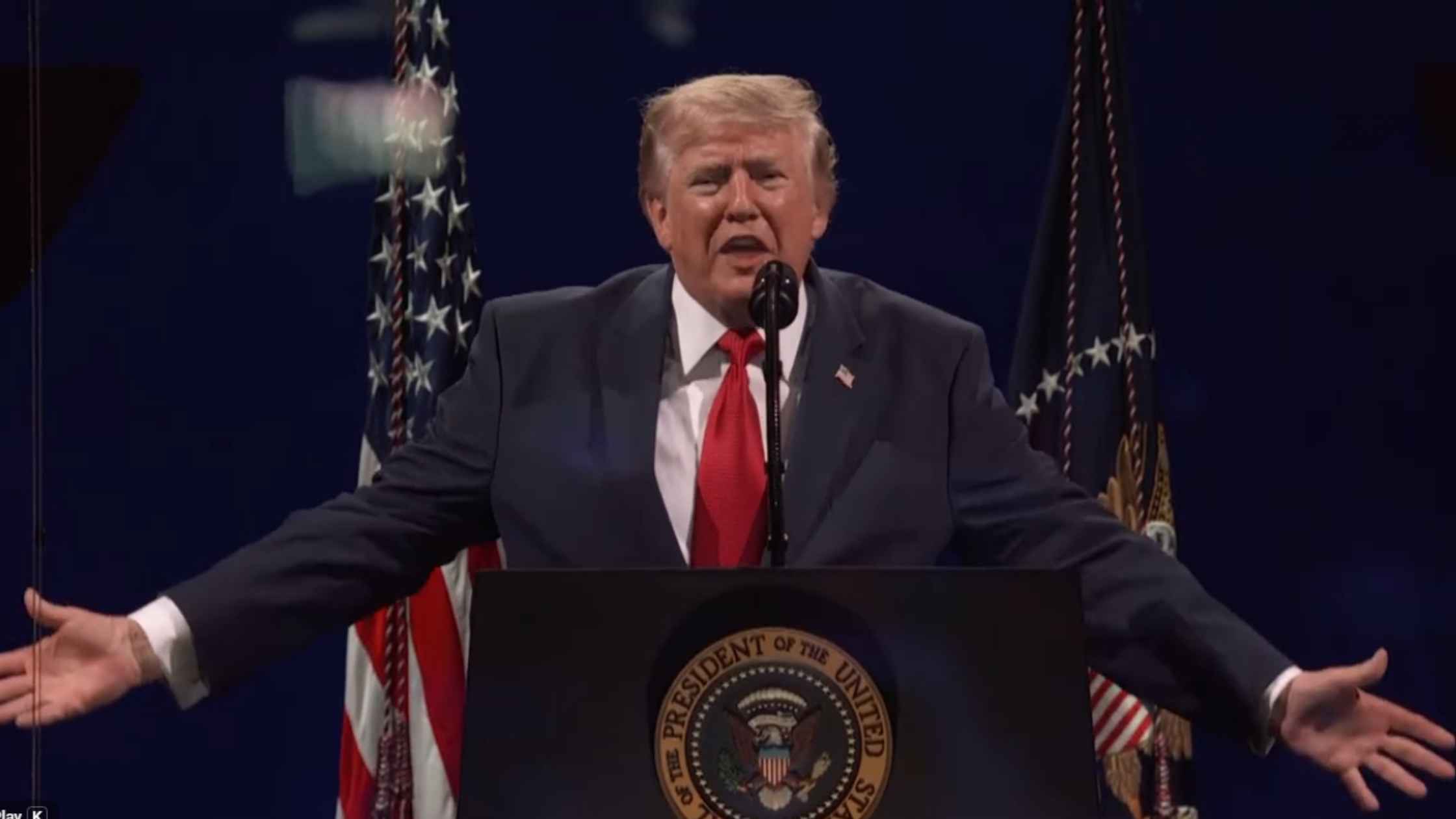
America 250 Keynote Address
Donald Trump delivers the keynote address at America 250. Read the transcript here.
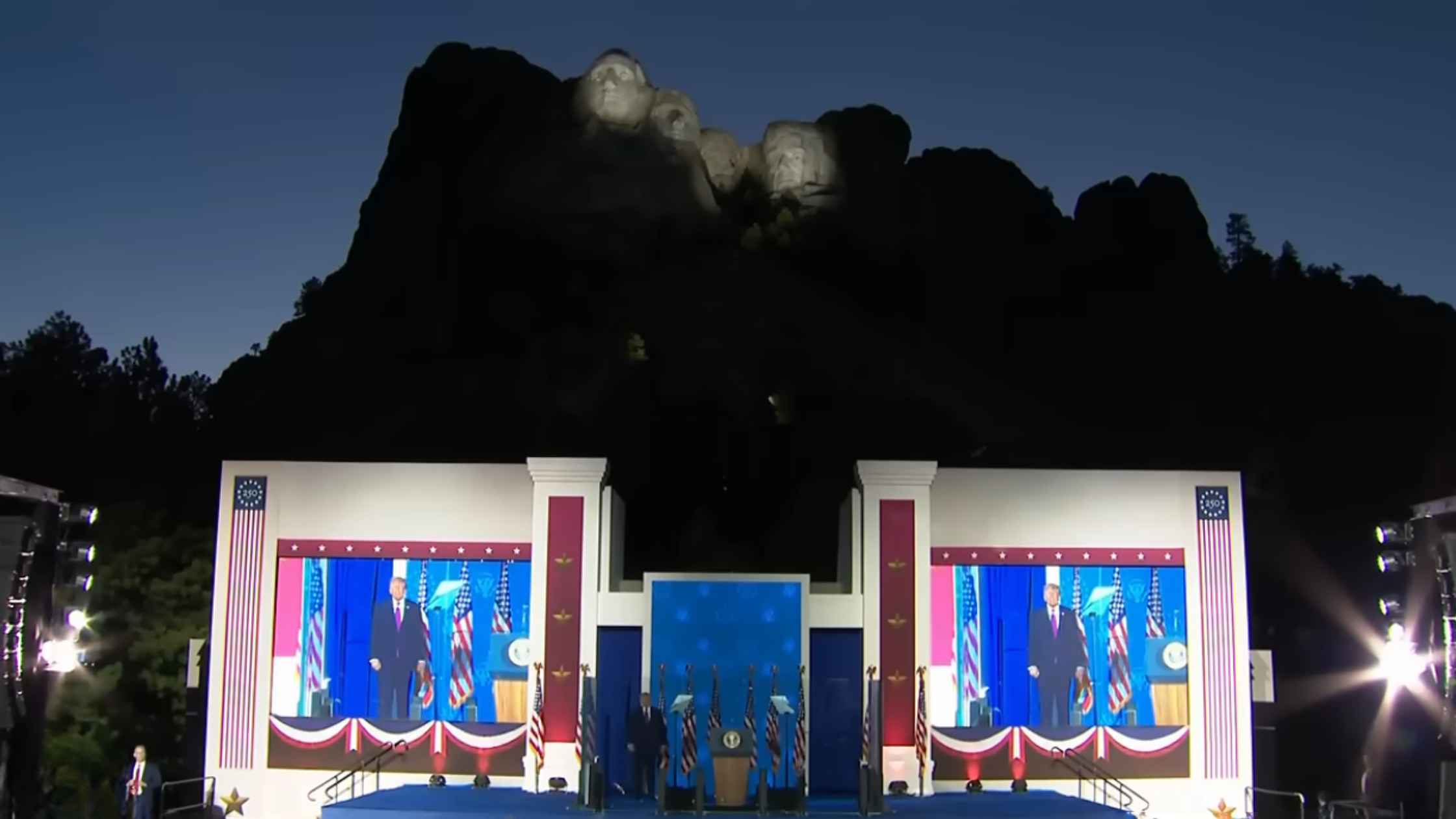
Mount Rushmore Speech
Donald Trump speaks at Mount Rushmore on the eve of America 250. Read the transcript here.

Northern Border Hearing
The Subcommittees on Border Security and Enforcement and Counterterrorism and Intelligence hold a hearing on the U.S. Northern Border. Read the transcript here.
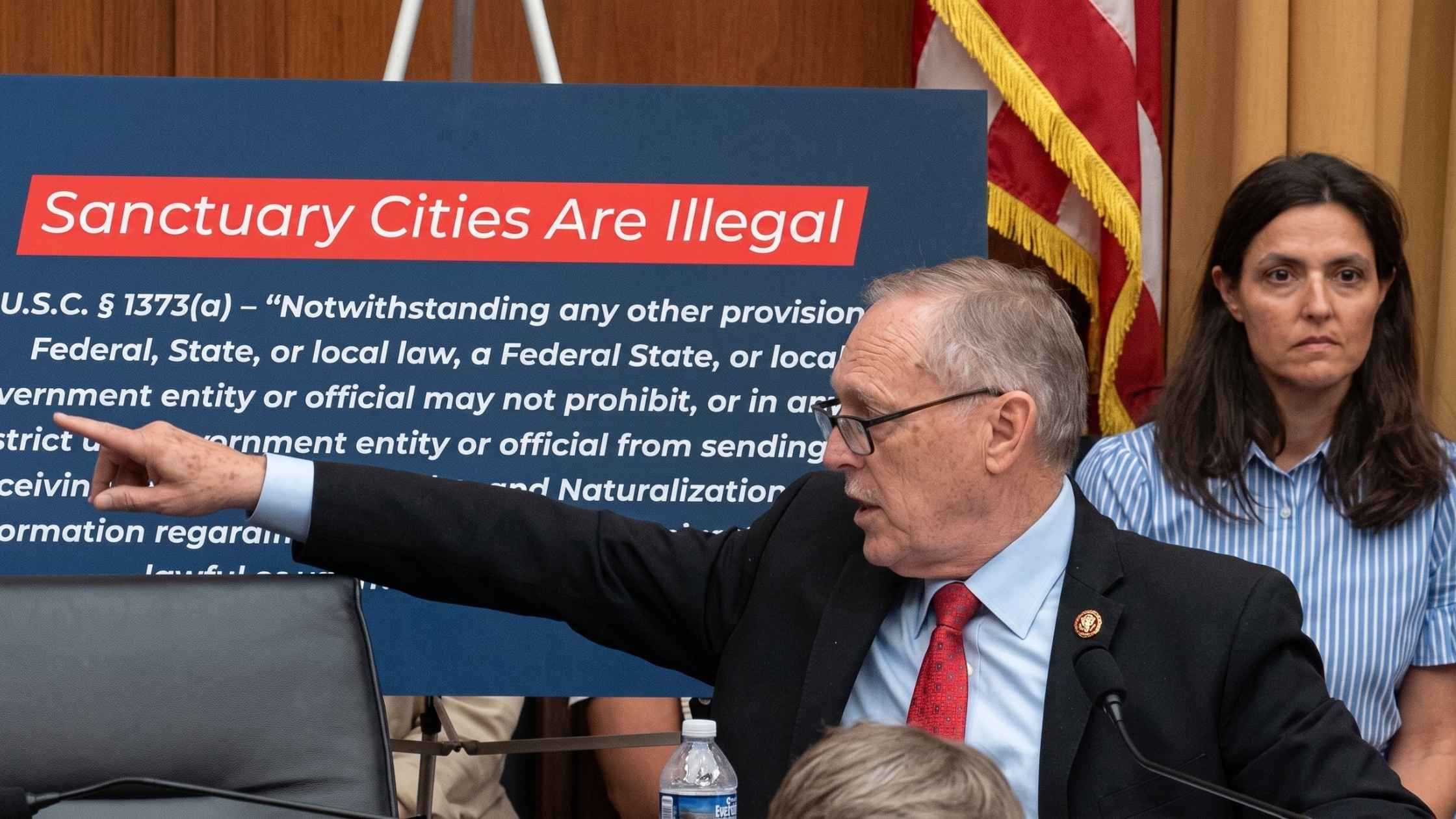
Sanctuary Cities Congressional Hearing
House Judiciary Subcommittee on Immigration Integrity, Security, and Enforcement holds a hearing on Sanctuary City policies. Read the transcript here.

Tren de Aragua Press Conference
Todd Blanche and Kash Patel hold a press conference on the takedown of the Venezuela Gang, Tren de Aragua. Read the transcript here.

Actor Sean Astin Testifies in IP Protection Hearing
Actor Sean Astin testifies before Congress about Intellectual Property protection in the Digital Age. Read the transcript here.
MKUltra Congressional Hearing
Lawmakers probe the CIA's MKUltra and Mind Control programs in House Oversight Committee. Read the transcript here.

Right to Fix Executive Order
Donald Trump signs an executive order pertaining to auto repairs. Read the transcript here.

Murdaugh Retrial Pretrial Hearing
Alex Murdaugh is back in court for a pretrial hearing ahead of his retrial. Read the transcript here.

House DHS Hearing
DHS Secretary Markwayne Mullin testifies before the House Appropriations Committee. Read the transcript here.

House Hearing on Medicaid Fraud
The House Energy & Commerce Subcommittee on Oversight and Investigations holds a hearing on Medicaid fraud. Read the transcript here.
Subscribe to The Rev Blog
Sign up to get Rev content delivered straight to your inbox.