Rev’s Transcript Library
Explore our extensive collection of free transcripts from political figures and public events. Journalists, students, researchers, and the general public can explore transcripts of speeches, debates, congressional hearings, press conferences, interviews, podcasts, and more.
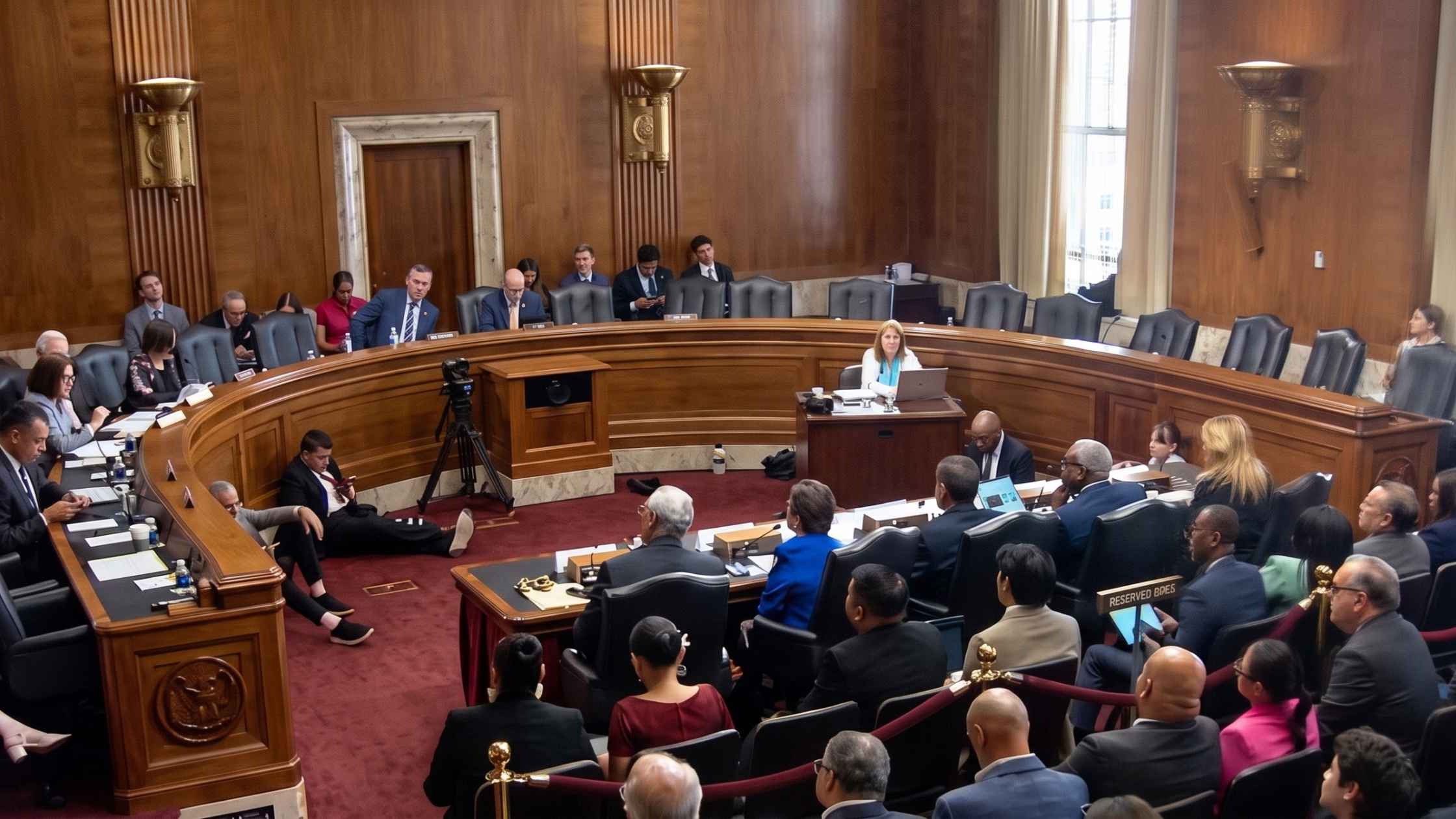
American Citizenship Congressional Hearing
The Senate Judiciary Subcommittee on the Constitution holds a hearing on American citizenship. Read the transcript here.

Mark Rutte at the White House
Donald Trump meets with visiting NATO Secretary-General Mark Rutte at the White House. Read the transcript here.

USPS Congressional Hearing
Postmaster General David Steiner testifies before the Senate Homeland Security & Governmental Affairs Committee. Read the transcript here.

House Rules Committee Budget Hearing
The House Rules Committee holds a hearing on the State Department budget. Read the transcript here.
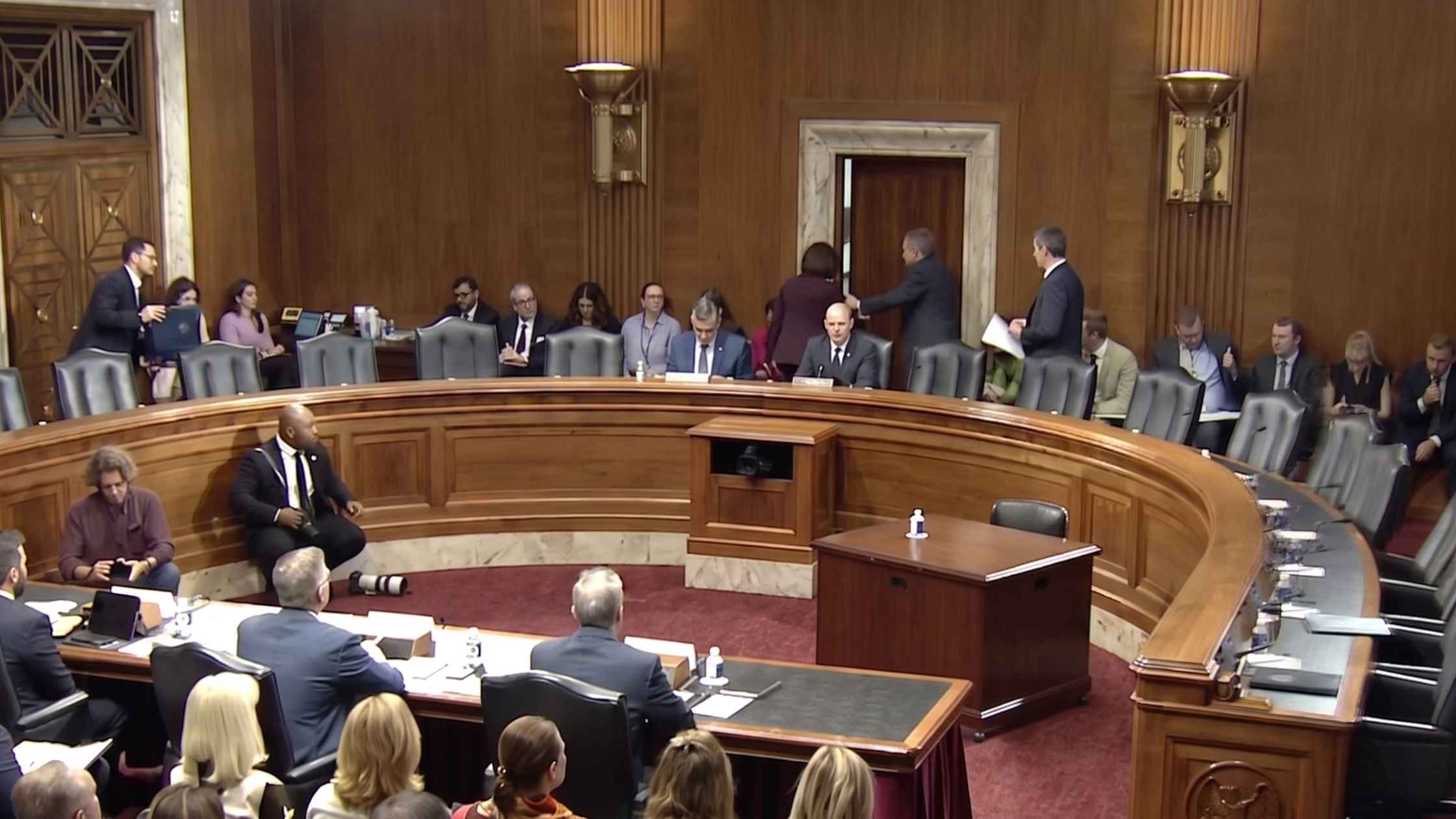
Senate Energy Committee Hearing
The Senate Energy Committee holds a hearing on pending nominations. Read the transcript here.
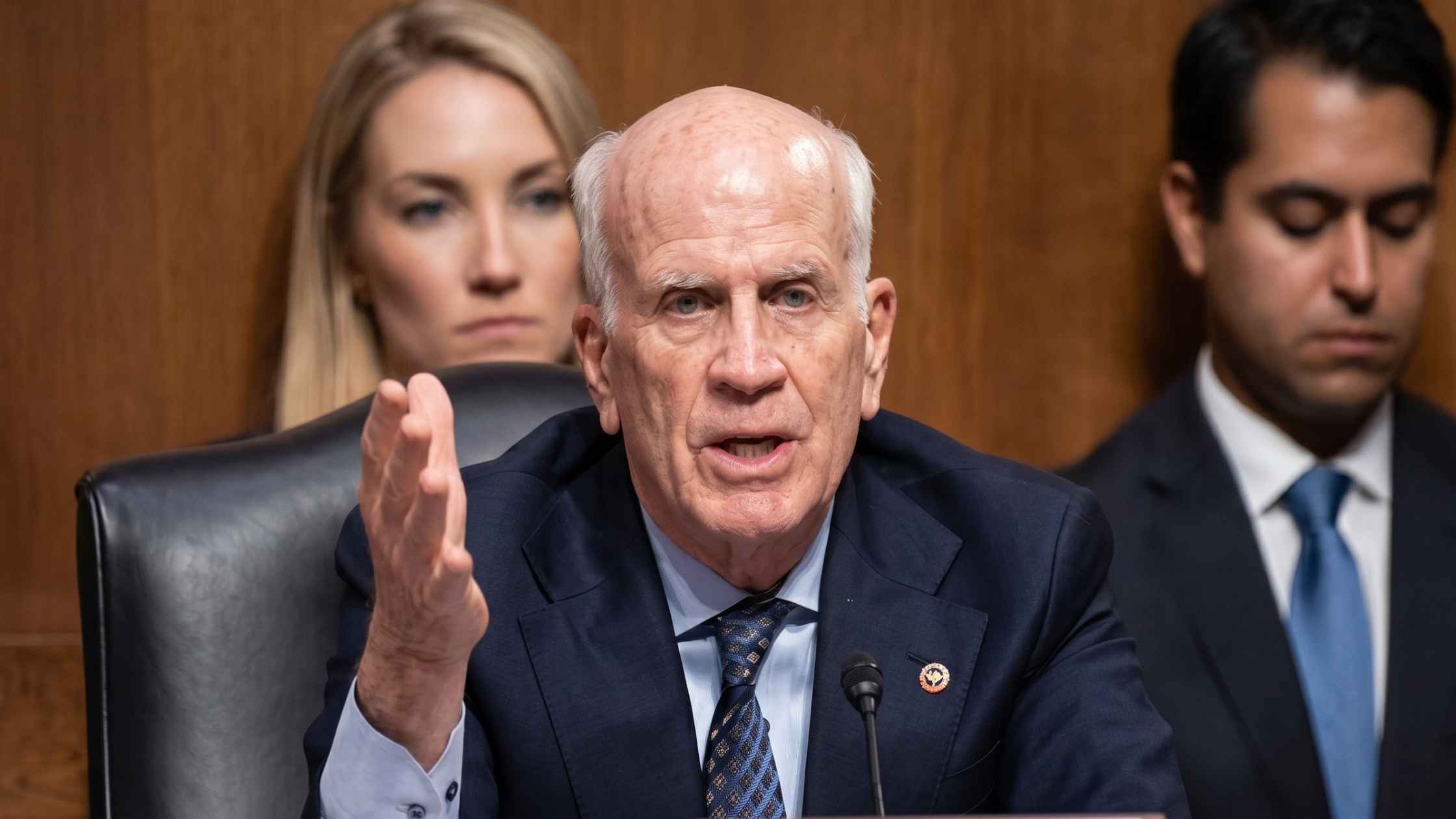
Senate Banking Committee Hearing On Affordability
The Senate Banking Committee holds a hearing on lowering costs and affordability. Read the transcript here.
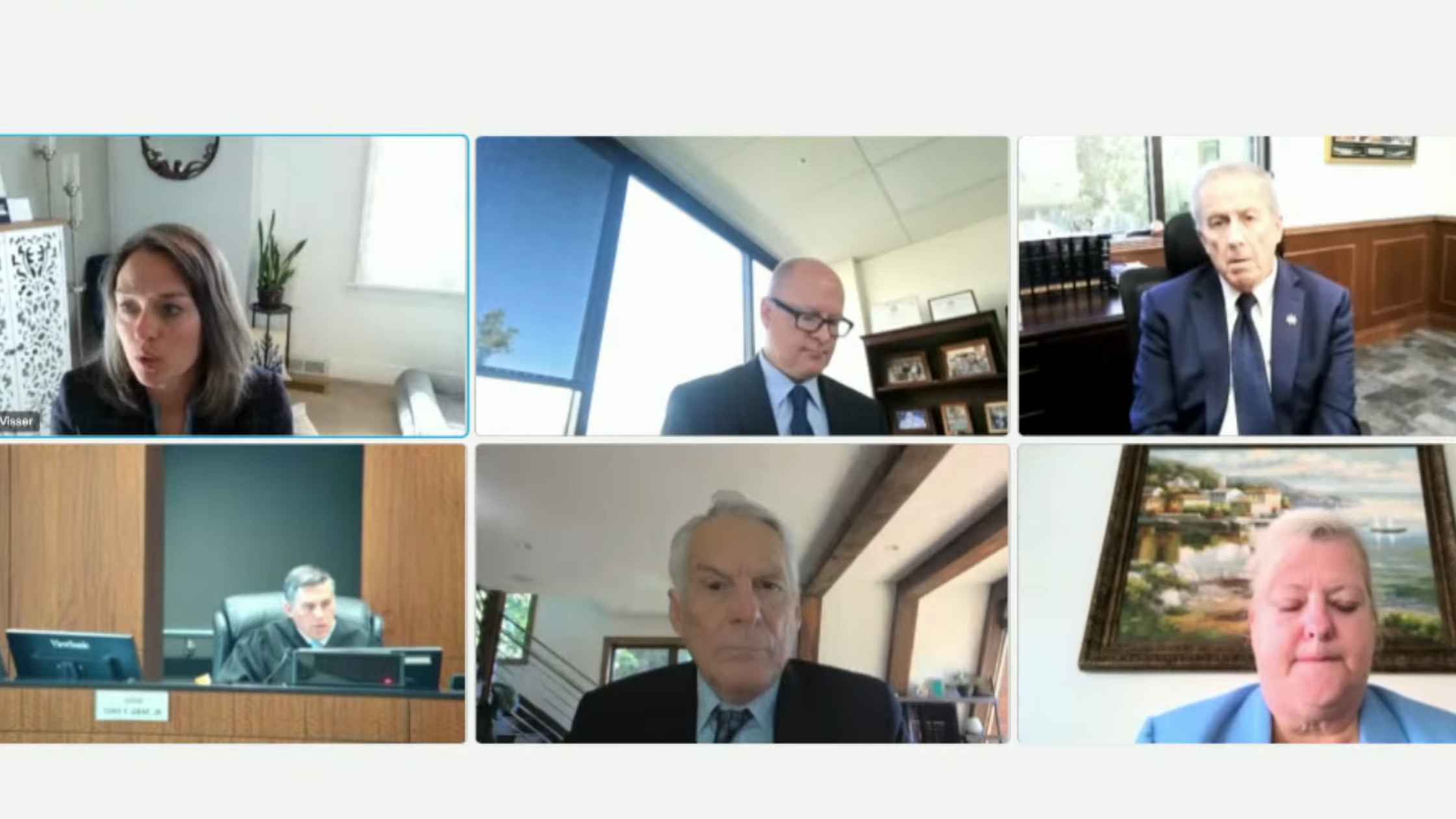
Tyler Robinson Comtempt Hearing
Hearing to determine if prosecutors will be held in contempt for comments made about the bullet that killed Charlie Kirk. Read the transcript here.

Senate Foreign Relations Committee Confirmation
U.S. Ambassador to Jamaica nominee Kari Lake testifies before the Senate Foreign Relations Committee for her confirmation hearing. Read the transcript here.
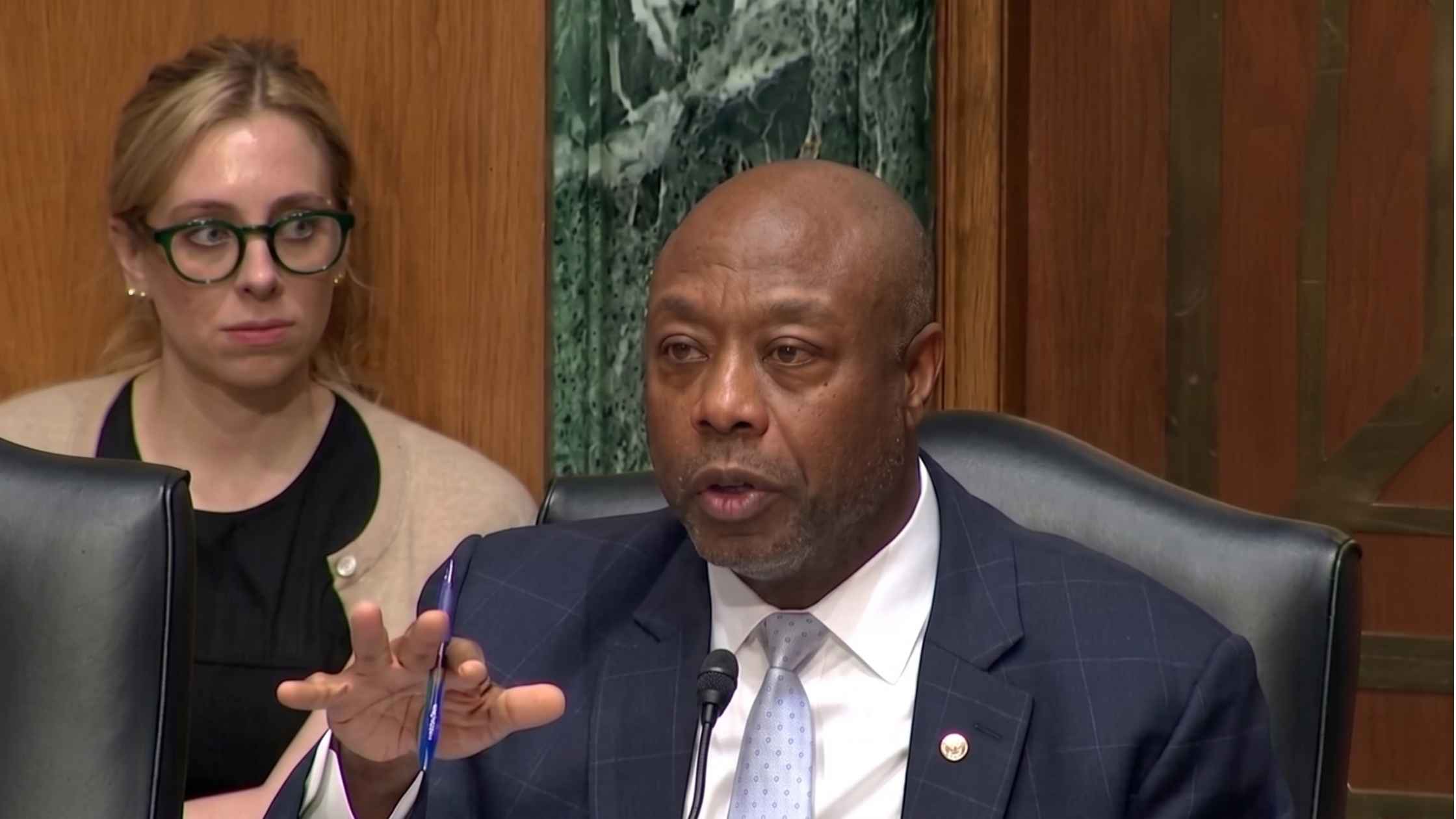
Senate Energy Committee Hearing
Senate Energy Committee Hearing on United States Territories. Read the transcript here.
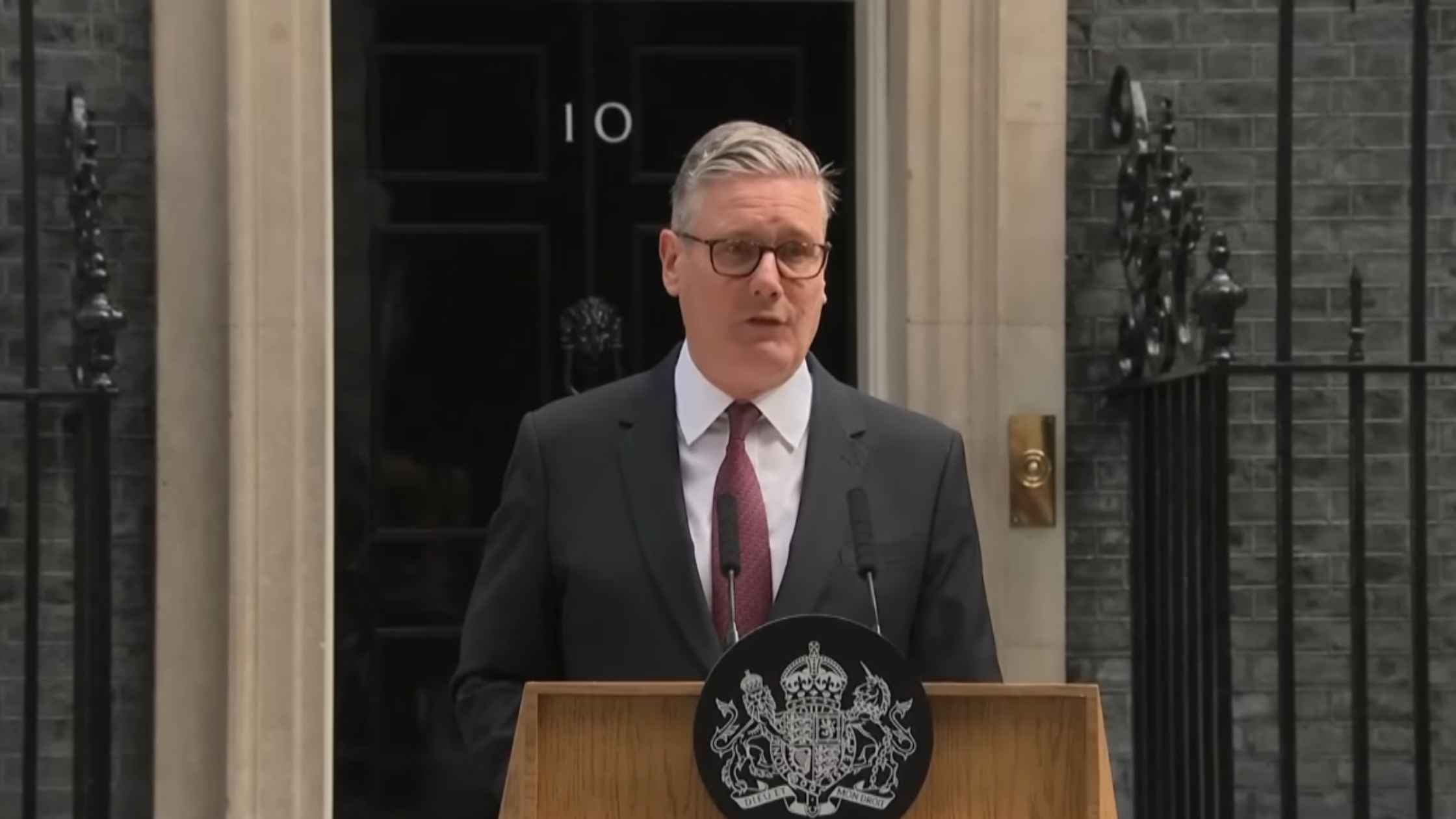
Keir Starmer Resigns
Keir Starmer announces his resignation as UK Prime Minister. Read the transcript here.

Trump and Macron speak at G7 Summit
Donald Trump meets with French President Emmanuel Macron during the G7 summit. Read the transcript here.

Gavin Newsom Statement on DOJ Investigation
California Governor Gavin Newsom responds to the DOJ's investigation of him and his wife. Read the transcript here.
Subscribe to The Rev Blog
Sign up to get Rev content delivered straight to your inbox.