




Rev’s Transcript Library
Explore our extensive collection of free transcripts from political figures and public events. Journalists, students, researchers, and the general public can explore transcripts of speeches, debates, congressional hearings, press conferences, interviews, podcasts, and more.

Treasury Congressional Hearing
U.S. Treasury Secretary Scott Bessent testifies before the Senate Appropriations Committee. Read the transcript here.

Commerce Department Budget Hearing
Howard Lutnick testifies on the Commerce Department budget request before the Senate. Read the transcript here.

Supreme Court Greencard Hearing
Supreme Court hears arguments on the rights of green card holders. Read the transcript here.

NASA Budget Hearing
NASA Administrator Jared Isaacman testifies on the 2027 budget proposal for the space agency. Read the transcript here.
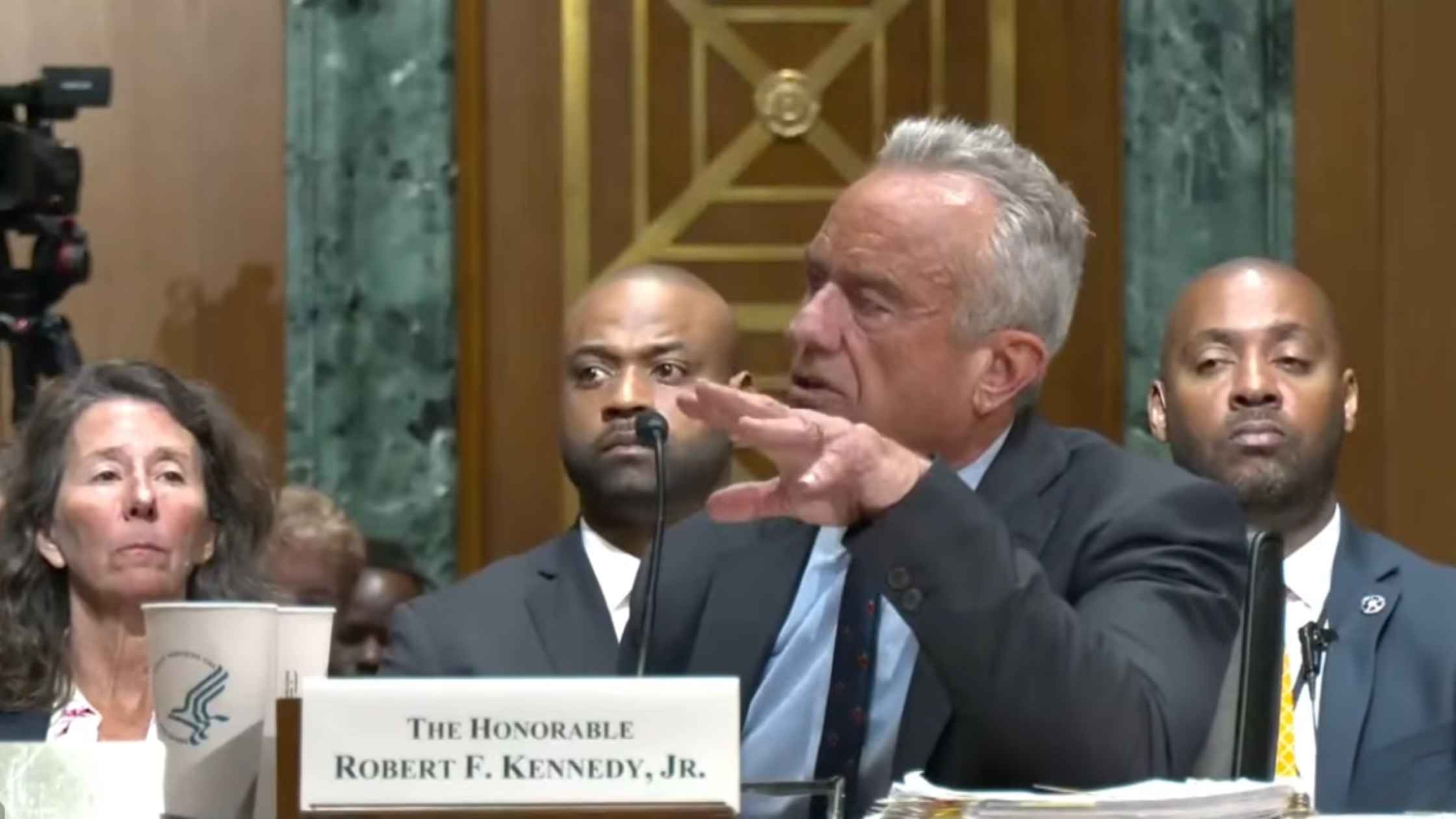
HHS Budget Hearing
RFK Jr. testifies on HHS budget request before Senate Finance Committee. Read the transcript here.

DOJ Announces SPLC Indictment
Acting Attorney General Todd Blanche and FBI Director Kash Patel announce an indictment against the Southern Poverty Law Center. Read the transcript here.
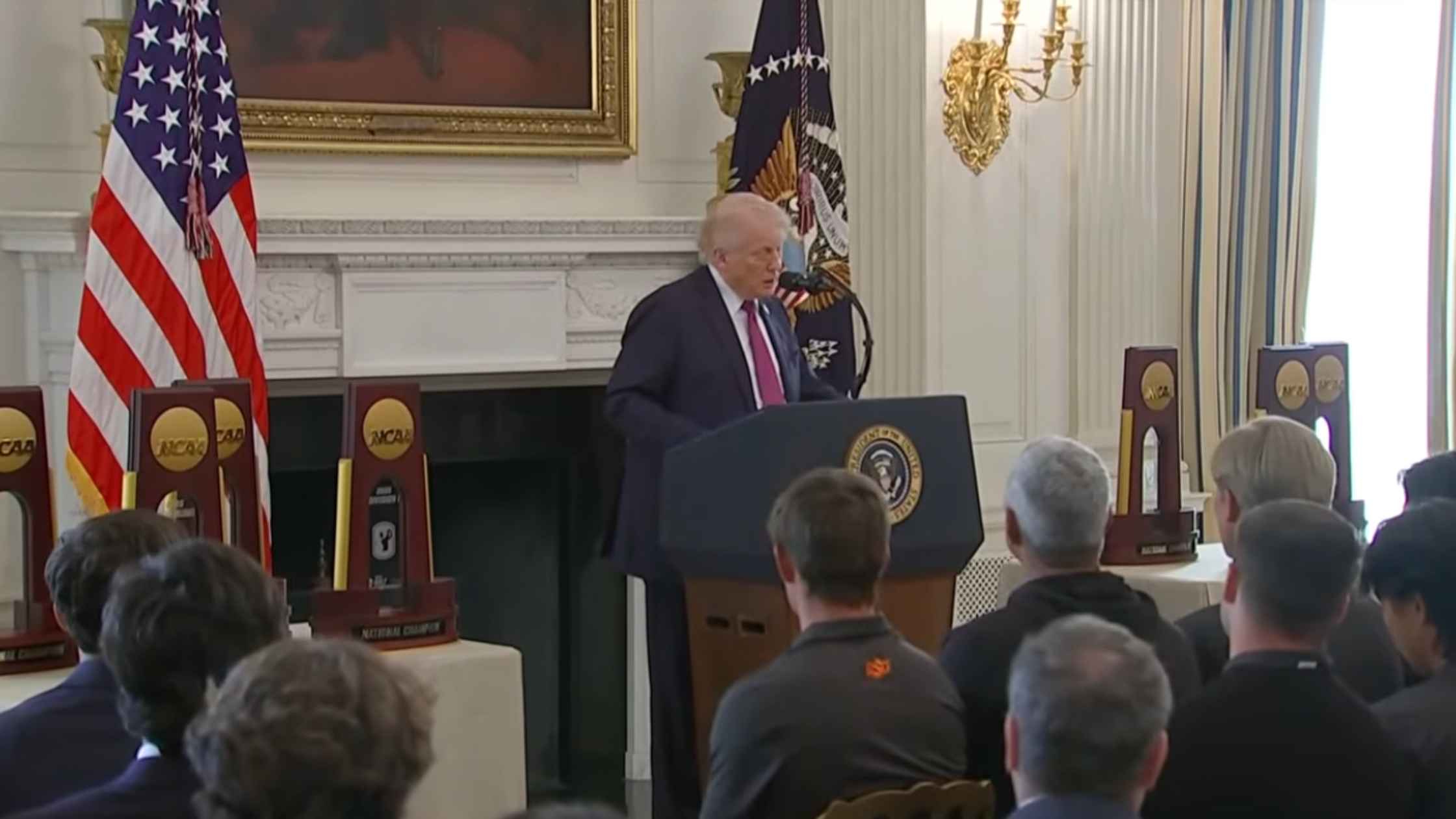
NCAA Champions at the White House
Donald Trump hosts NCAA champions at the White House. Read the transcript here.

Warsh Confirmation Hearing
Fed Chair nominee Kevin Warsh testifies before the Senate Banking Committee at a confirmation hearing. Read the transcript here.
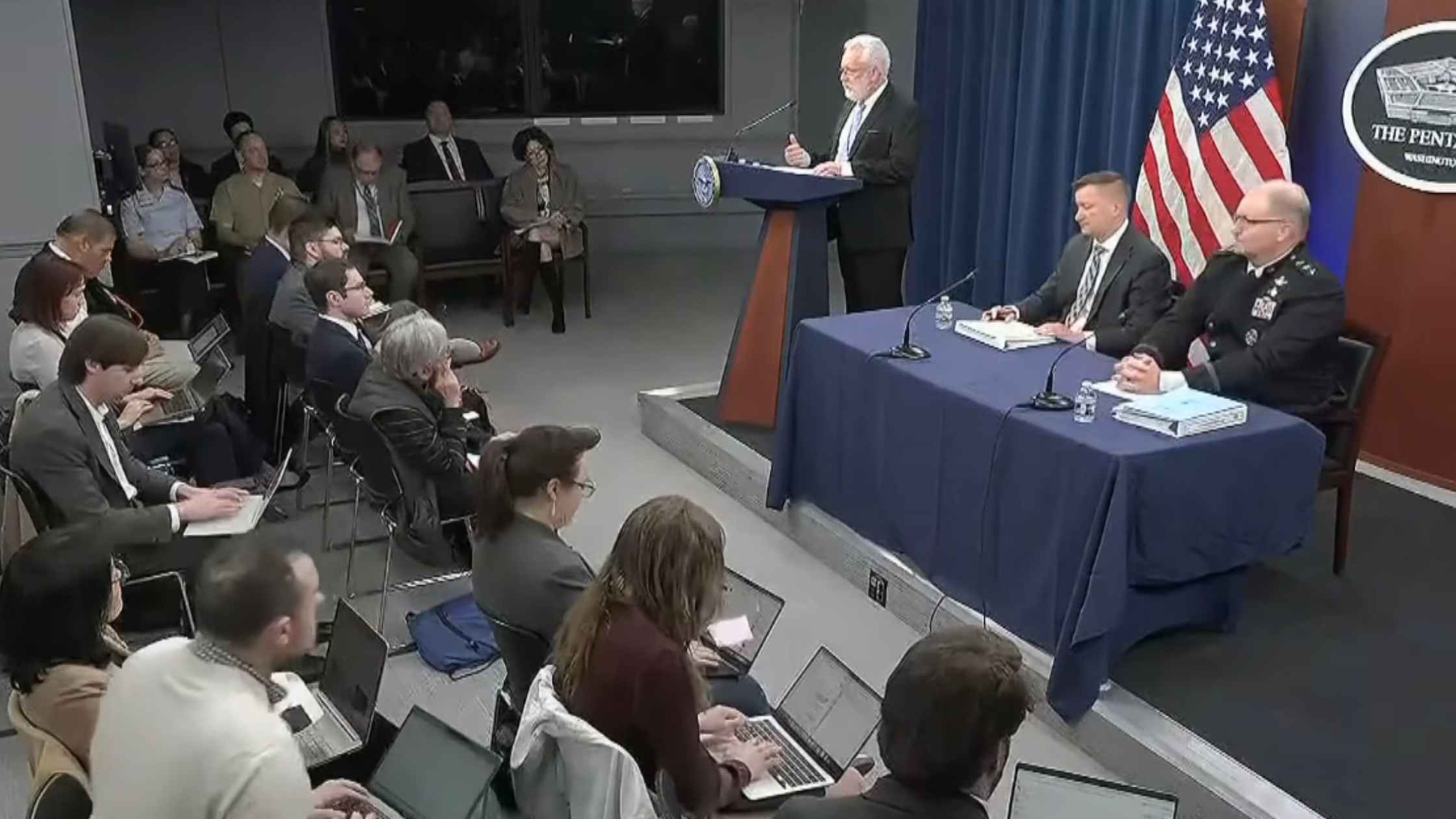
Pentagon Budget Briefing
Pentagon officials give a press briefing to outline their budget request for the coming year. Read the transcript here.
Subscribe to The Rev Blog
Sign up to get Rev content delivered straight to your inbox.