




Rev’s Transcript Library
Explore our extensive collection of free transcripts from political figures and public events. Journalists, students, researchers, and the general public can explore transcripts of speeches, debates, congressional hearings, press conferences, interviews, podcasts, and more.

Nordic-Canada Summit
Prime ministers of Iceland, Sweden, Canada, Norway, Denmark, and Finland hold a news conference following the Nordic-Canada Summit in Oslo. Read the transcript here.

Military Commanders Testify
Top military commanders testify on defense readiness before the U.S. Senate Committee on Armed Services. Read the transcript here.
Pirro Press Conference on Powell
Jeanine Pirro holds a press conference on the criminal investigation of Federal Reserve Chair Jerome Powell. Read the transcript here.
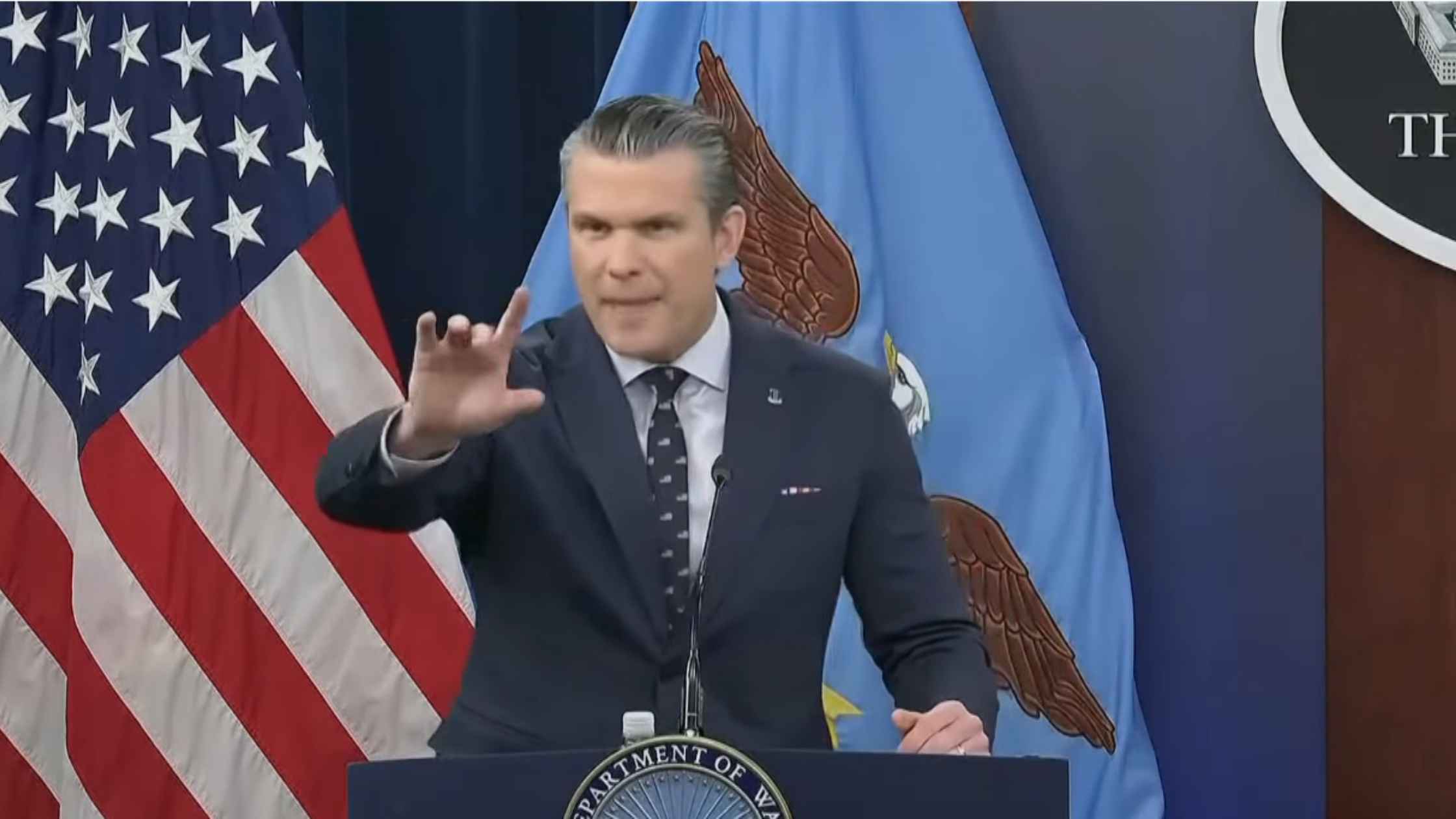
Pentagon Press Briefing for 3/13/26
Pete Hegseth delivers a Pentagon press briefing for 3/13/26. Read the transcript here.
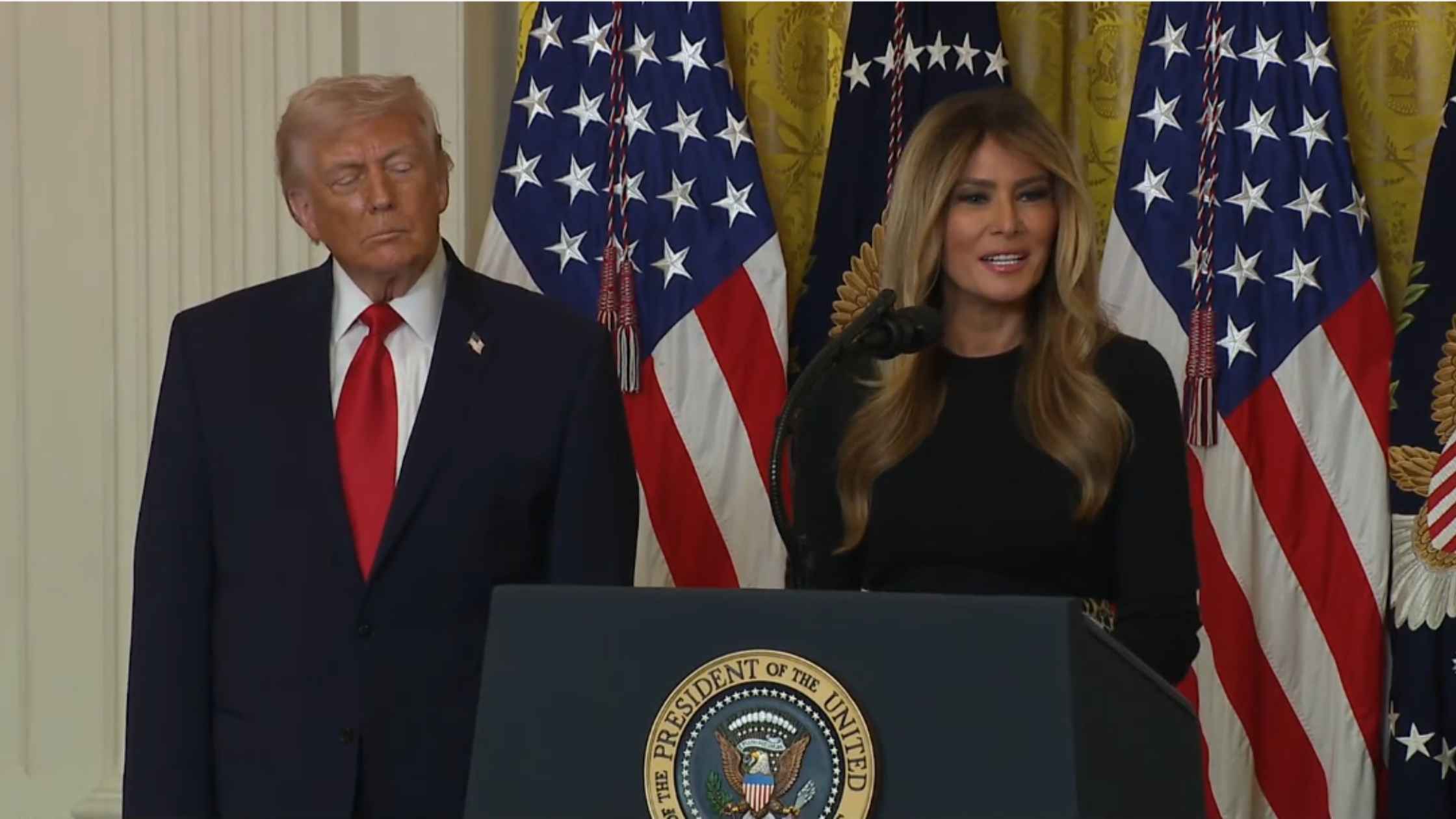
Women's History Month Event
Donald and Melania Trump participate in a Women's History Month event. Read the transcript here.
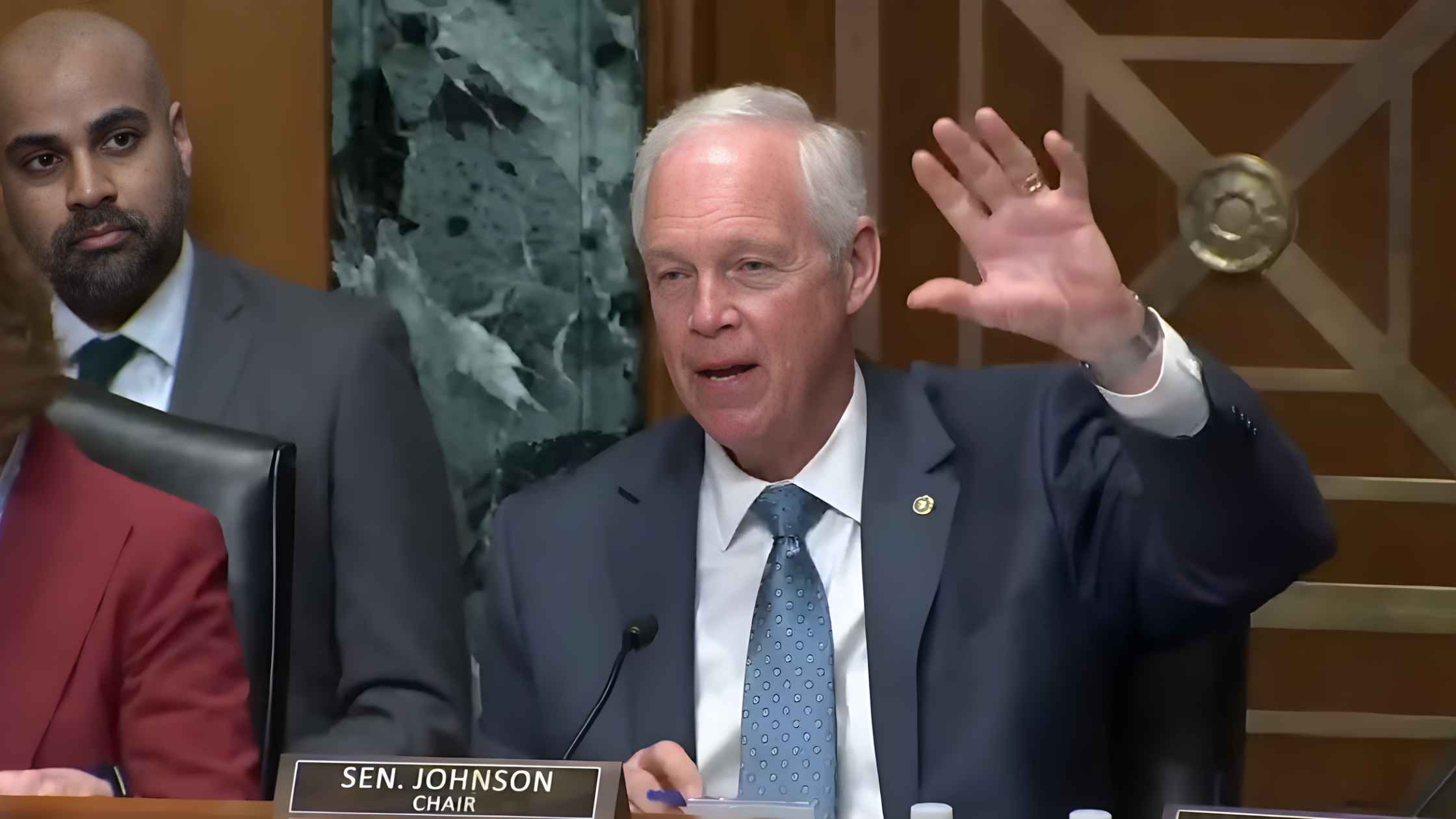
Senate Finance Committee Hearing
The Senate Finance Committee examines the U.S. financial outlook for the next decade. Read the transcript here.

Trump Rally in Kentucky
Donald Trump delivers remarks on the economy at Verst Logistics Contract Packaging Facility in Hebron, Kentucky. Read the transcript here.

Altman speaks at BlackRock's US Infrastructure Summit
OpenAI CEO Sam Altman speaks at BlackRock's U.S. Infrastructure Summit in Washington, D.C. Read the transcript here.
Senate Citizenship Hearing
Senate panel examines birthright citizenship rights. Read the transcript here.
Subscribe to The Rev Blog
Sign up to get Rev content delivered straight to your inbox.